Material: medical titanium alloy
Diameter: 1.6mm
Product specification
|
Item No. |
Specification |
|
10.07.0516.006115 |
1.6*6mm |
|
10.07.0516.007115 |
1.6*7mm |
Features & Benefits:
• used for orthodontic anchorage and intermaxilary ligation.
• the head of screw has two cross holes, easy to insert wire.
• square screw head design ensures better holding and torque force, easier to screw in.

Matching instrument:
medical drill bit φ1.4*5*95mm (for harder cortical bone)
orthodontic screw driver: SW2.4
broken nail extractorφ2.0
straight quick coupling handle
The method of ligation and fixation between small annular jaws is suitable for:
1. Single linear fracture of mandible body without obvious displacement.
2. The benign tumor of the mandibular body or chin was removed and bone grafted immediately.
3. Comprehensive auxiliary fixation of mandibular defects after firearm injury by bone grafting.
Early reduction, fixation and functional motor therapy are the three principles for the definitive treatment of limb fractures.Jaw bone fracture treatment principle, have their similarities and differences, the upper jaw fractures, because its the muscles of the bone surface attachment, in addition to the wing of internal and external muscle, more for the expression of some weak muscle, as long as the teeth can return to normal relations, judge fracture section have been reset, then select the fixed methods of fracture fixed in the base of skull.And mandible fracture because of the strong masticatory muscles pull can cause obvious dislocation, the method of fixed jaw fracture must be more stable, at the same time take into account the temporomandibular joint of early functional exercise, active and painless activity can promote the blood supply of bone and soft tissue, synovial fluid promotes the articular cartilage nutrition, combined with partial weight-bearing, prevent muscle disuse atrophy, joint stiffness, etc., therefore, the treatment of mandibular fracture guidelines, aspires to the three principles.
Restoring occlusion is the goal of treatment. Jawbone fracture is different from long tube fracture, its significant particularity, that is, there is a row of arch dentition on the body of the jaw, and the formation of a normal occlusal relationship between the upper and lower mandibles, managing the masticatory function.Whether the occlusal relationship of upper and lower teeth can be restored is one of the most important indicators to evaluate the treatment effect of jaw fracture.The teeth on the bone segment are often used as a support or anchor base for reduction and fixation by ligating arch splints or other intraoral splints.In the case of non-firearm injuries, it is recommended that the teeth at the fracture line should be preserved as far as possible.If the root is broken, the tooth is extremely loose, the fracture line is impacted through the third mandibular molar or the tooth is embedded, the tooth should be removed.For jaw firearm injury, more to cherish the alveolar process of the remaining teeth, should be restored and retained by every means possible, the crown is broken but there is a strong root, especially after the fracture section of the strong root, can be used for root canal treatment, but also conducive to as a post nail or cover the fixation of the brackets.
Up to 50–70% of people who survive traffic accidents suffer from facial trauma. In most developed countries, violence from other people has replaced vehicle collisions as the main cause of maxillofacial trauma; In the case of developing countries traffic accidents are still the major cause. Seatbelt and airbag have been used to reduce the incidence of maxillofacial trauma, but fractures of the mandible, namely the jawbone, are not decreased by these protective measures. Using of motorcycle helmets can decrease maxillofacial trauma efficiently.
Maxillofacial fractures are distributed in a fairly normal curve by age, with a peak incidence occurring between ages 20 and 40, and children under 12 suffering only 5–10% of all maxillofacial fractures. Most maxillofacial trauma in children involves lacerations and soft tissue injuries. There is a lower proportion of cortical bone to cancellous bone in children's faces, poorly developed sinuses make the bones stronger, and fat pads provide protection for the facial bones.
Head and brain injuries are commonly associated with maxillofacial trauma, particularly that of the upper face; brain injury occurs in 15–48% of people with maxillofacial trauma. Coexisting injuries can affect treatment of facial trauma; for example they may be emergent and need to be treated before facial injuries. People with trauma above the level of the collar bones are considered to be at high risk for cervical spine injuries (spinal injuries in the neck) and special precautions must be taken to avoid movement of the spine, which could worsen a spinal injury.
-
orthognathic 1.0 sagittal split fixed 4 holes p...
-
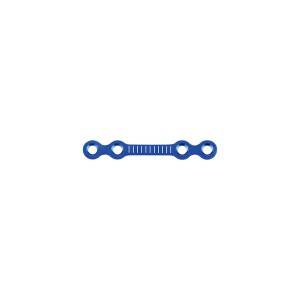
locking maxillofacial micro Y plate
-
maxillofacial reconstruction straight plate
-
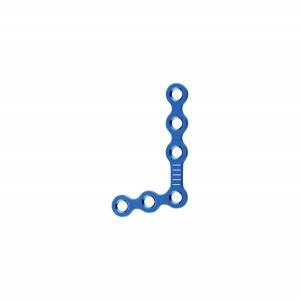
orthognathic 1.0 L palte 6 holes
-
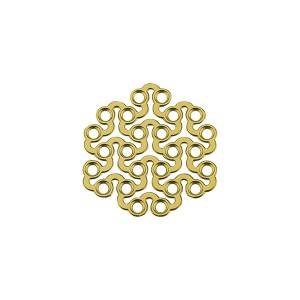
minimally invasive titanium mesh anodized
-
maxillofacial trauma mini straight bridge plate